

The opioid epidemic continues to be a major public health problem in the United States. The number of people seeking  treatment for opioid abuse is now greater than for alcohol abuse. In the period from 2006 to 2008, the number of deaths related to opioid overuse surpassed the death rate from motor vehicle accidents. According to the Centers for Disease Control (CDC), in 2017, more than 70,000 people lost their life due to opioids making opioid overuse the leading source of injury-related death in the country. More than 17% of Americans had at least one opioid prescription filled with an average of 3.4 opioid prescriptions dispensed per patient.
treatment for opioid abuse is now greater than for alcohol abuse. In the period from 2006 to 2008, the number of deaths related to opioid overuse surpassed the death rate from motor vehicle accidents. According to the Centers for Disease Control (CDC), in 2017, more than 70,000 people lost their life due to opioids making opioid overuse the leading source of injury-related death in the country. More than 17% of Americans had at least one opioid prescription filled with an average of 3.4 opioid prescriptions dispensed per patient.
The White House Council of Economic Advisers estimated the economic burden to be $504 billion in 2015. More narrowly constructed estimates find cost burdens as high as $95 billion in 2016 as reported by the American Enterprise Institute.
 Few communities are untouched by the opioid epidemic, which kills an average of 130 people each day. West Virginia has the highest rates (57.8 per 100,000), followed by Ohio (46.3 per 100,000), Pennsylvania (44.3 per 100,000), the District of Columbia (44.0 per 100,000), and Kentucky (37.2 per 100,000). Oregon and Colorado were among the highest rates of painkiller misuse in 2017. Prescription drugs and illicit opioids played a role in 68% of cases. Fentanyl, a synthetic opioid that is 50 to 100 times more potent than morphine, is responsible for an 800% increase in 4 years! In its prescription variety, fentanyl is known as Duragesic®, Sublimaze®, and Actiq®. On the illegal market, the drug is known as Apache, China Girl, China White, Dance Fever, Friend, Goodfellas, Jackpot, Murder 8, and Tango & Cash. Fentanyl is often mixed with other drugs, such as heroin, methamphetamine, or cocaine often unbeknownst to the user.
Few communities are untouched by the opioid epidemic, which kills an average of 130 people each day. West Virginia has the highest rates (57.8 per 100,000), followed by Ohio (46.3 per 100,000), Pennsylvania (44.3 per 100,000), the District of Columbia (44.0 per 100,000), and Kentucky (37.2 per 100,000). Oregon and Colorado were among the highest rates of painkiller misuse in 2017. Prescription drugs and illicit opioids played a role in 68% of cases. Fentanyl, a synthetic opioid that is 50 to 100 times more potent than morphine, is responsible for an 800% increase in 4 years! In its prescription variety, fentanyl is known as Duragesic®, Sublimaze®, and Actiq®. On the illegal market, the drug is known as Apache, China Girl, China White, Dance Fever, Friend, Goodfellas, Jackpot, Murder 8, and Tango & Cash. Fentanyl is often mixed with other drugs, such as heroin, methamphetamine, or cocaine often unbeknownst to the user.
The CDC has issued a Guideline for Prescribing Opioids for Chronic Pain, which focuses on 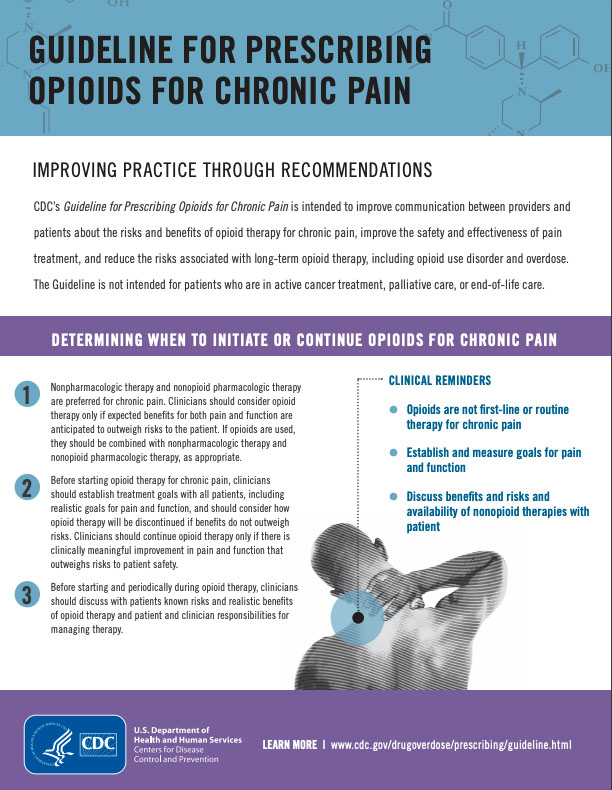
- Determining when to initiate or continue opioids for chronic pain
- Opioid selection, dosage, duration, follow-up, and discontinuation
- Assessing risk and addressing harms of opioid use
The Guideline stipulates that nonpharmacologic therapy, including physical therapy, and nonopioid pharmacologic therapy are preferred for chronic pain,” but does not include any further suggestions.
State governments have also issued guidelines, but few, if any include concrete recommendations for nonpharmacologic therapy. The Maryland Opioid Overdose Prevention Plan, as an example, addresses opioid prescription monitoring, access to substance use disorder treatment and recovery services, providing clinical education and training for healthcare providers, and increasing access to naloxone, but fails to include alternative options for chronic pain management, such as physical therapy.
In 2018, the American Physical Therapy Association (APTA) issued a white paper on “Beyond Opioids: How Physical Therapy Can Transform Pain Management to Improve Health,” which advocates for a central role of physical therapy in the overall management of chronic pain. Physical therapists may design individualized treatment programs combining the most appropriate techniques, including but not limited to exercise, manual therapy, and patient education. The APTA also released a fact sheet “Providing a Safe Alternative to Opioids: Research on Pain Management.”
On February 20, 2018, National Public Radio’s program “All Things Considered” reported that the Emergency Room of St. Joseph’s University Medical Center in Paterson, N.J. saw a 58 percent drop in opioid prescriptions in one year after implementing an alternative program. Many patients coming to the ER have muscle pain, which in the past was commonly treated with Percocet (a combination of acetaminophen and oxycodone) or Vicodin (a combination of acetaminophen and hydrocodone). Since the new program has been implemented, patients with muscle pain are treated with trigger point dry needling! Other treatment options include lidocaine patches, nitrous oxide (laughing gas), and even a harpist playing soothing music.
 Other emergency departments have since followed the New Jersey program, i.e., the Department of Emergency Medicine at the Community Hospital of Monterey in California invited Myopain Seminars to teach manual trigger point therapy to the clinical staff. Physicians, nurses, and physical therapists attended our Manual Trigger Point Therapy courses taught by Stew Wild. Just a few months after completing the MTT courses, the team published a case report in the journal Clinical Practice and Cases in Emergency Medicine (2019; 3(3):259-261). The case involved a 42-year-old female who presented to the ED with atraumatic back pain. Her pain was thought to be myofascial, and the ED physician obtained a physical therapy consultation. Diagnosing the patient with quadratus lumborum spasm, the physical therapist treated her in the ED using manual trigger point therapy and completely relieved her pain without requiring any medications. According to the report, “manual trigger point therapy is an effective means of treating muscle spasm without using needles or potentially addictive medications, and therefore represents a novel option for non-opioid ED pain management.” Besides, Roldan reported that “traditionally, the emergency physician is not trained to diagnose and treat myofascial pain syndrome (MPS), and many patients with MPS have received less than optimal management of this condition in the ED.”
Other emergency departments have since followed the New Jersey program, i.e., the Department of Emergency Medicine at the Community Hospital of Monterey in California invited Myopain Seminars to teach manual trigger point therapy to the clinical staff. Physicians, nurses, and physical therapists attended our Manual Trigger Point Therapy courses taught by Stew Wild. Just a few months after completing the MTT courses, the team published a case report in the journal Clinical Practice and Cases in Emergency Medicine (2019; 3(3):259-261). The case involved a 42-year-old female who presented to the ED with atraumatic back pain. Her pain was thought to be myofascial, and the ED physician obtained a physical therapy consultation. Diagnosing the patient with quadratus lumborum spasm, the physical therapist treated her in the ED using manual trigger point therapy and completely relieved her pain without requiring any medications. According to the report, “manual trigger point therapy is an effective means of treating muscle spasm without using needles or potentially addictive medications, and therefore represents a novel option for non-opioid ED pain management.” Besides, Roldan reported that “traditionally, the emergency physician is not trained to diagnose and treat myofascial pain syndrome (MPS), and many patients with MPS have received less than optimal management of this condition in the ED.”
At Myopain Seminars, we are proud that we provide the best training in manual trigger point therapy and dry needling. Hopefully, other emergency room departments will follow the example of the Department of Emergency Medicine at the Community Hospital of Monterey and get trained in these viable alternatives to opioids.
{kind=link}