



The Intercostal Block: Clinical Value
Intercostal blocking is a palpation and grip technique used when performing trigger point dry needling of muscles over the chest wall. Described as securing the trigger point (TrP) between the index and middle fingers, wherein each finger is placed in the intercostal spaces adjacent to a rib upon which the TrP has been fixed [1], this intercostal blocking is done to “block” the needle from unintentionally advancing into the intercostal space. In contrast to the intercostal blocking technique, blindly needling muscles of the trunk have been documented to result in potentially deadly iatrogenic complications [2]. This palpation and grip may be used when dry needling muscles such as the rhomboids, the pectoralis major, the serratus anterior, or the inferior aspect of the latissimus dorsi.
Pneumothorax: Statistical Risk
Pneumothorax is a well-recognized (albeit rare) adverse event related to acupuncture or TrPDN over the chest wall [1-3]. The true incidence of dry-needling induced pneumothorax is difficult to calculate due to the probable under-reporting of minor events that do not require significant medical intervention. Clearer data may be obtained from socialized medical systems. The British National Health Service, for example, estimates the incidence of pneumothorax to be less than one in a million per procedure. Despite the favorable safety profile of trigger point dry needling, some patients. Non-clinical administrators and even non-dry-needling colleagues may express concern over dry needling safety in this area. After all, the statistical risk does not matter if you and your patient become the statistic.
Pneumothorax: Technical Risk
A 2014 article by Jung and colleagues in the Journal of Musculoskeletal Pain[4] challenges the widely held assumption that ultrasound guidance alone can render dry needling of the chest wall error-proof. Is ultrasound-guided dry needling promising or precarious? The answer is somewhat dependent upon the clinician at the end of the needle. In the case report, the clinician endeavored to dry needle intercostal musculature under ultrasound guidance — an incredibly dangerous lapse of clinical judgment — ultimately resulting in clinician-induced cardiac tamponade, pericardial effusion, and ultimately a 7-day patient hospital stay secondary to dry needling of the myocardium.
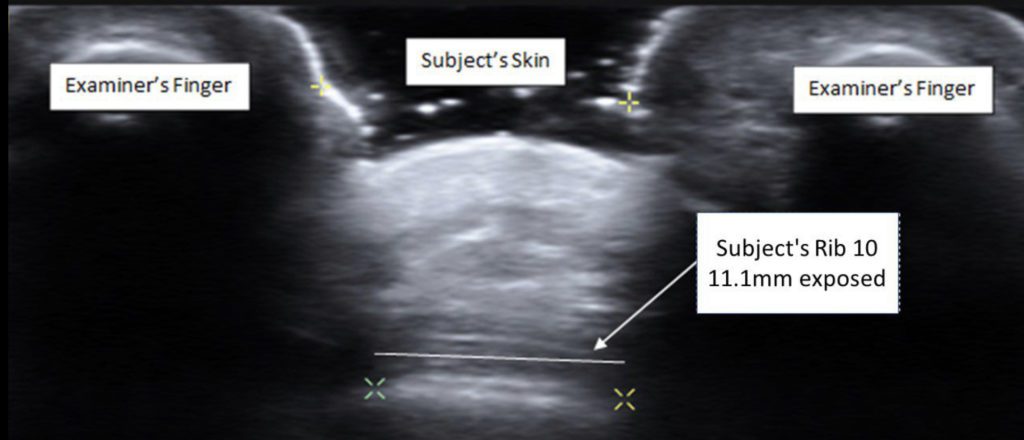 Trigger point dry needling of trunk musculature may pose a unique challenge to the clinician as safety is dependent upon the accuracy of palpating a thoracic rib as a “backstop” to prevent inadvertent puncture of the pleura. A recent study in the Journal of Bodywork and Movement Therapies reported that two physical therapists were accurate 73.3% of the time as verified with ultrasonography. As one might expect, the only subject characteristic or measurement that correlated with improved accuracy was a reduced muscle thickness [5]. Provided that the clinician accurately palpates the rib, another recent study in the American Journal of Interventional Radiology – co-authored by this author – reveals that when using the intercostal blocking technique, not only was a complete intercostal block achieved but an additional 6% – 13% of the rib was covered during maximal inhalation and exhalation respectively [6].
Trigger point dry needling of trunk musculature may pose a unique challenge to the clinician as safety is dependent upon the accuracy of palpating a thoracic rib as a “backstop” to prevent inadvertent puncture of the pleura. A recent study in the Journal of Bodywork and Movement Therapies reported that two physical therapists were accurate 73.3% of the time as verified with ultrasonography. As one might expect, the only subject characteristic or measurement that correlated with improved accuracy was a reduced muscle thickness [5]. Provided that the clinician accurately palpates the rib, another recent study in the American Journal of Interventional Radiology – co-authored by this author – reveals that when using the intercostal blocking technique, not only was a complete intercostal block achieved but an additional 6% – 13% of the rib was covered during maximal inhalation and exhalation respectively [6].
Clinical Impact & Current Best Practice
As performed by trained professionals on appropriate patients, trigger point dry needling using intercostal blocking is a safe and effective technique. The current best evidence suggests that safety may be maximized by first palpating with the patient in maximal inhalation and then administering dry needling in the respiratory mid-range. Furthermore, and in keeping with current Myopain Seminars philosophy and teaching, safety may be further optimized by inserting the dry needle midway between the examiner’s fingers at the distal interphalangeal joint at the center of the patient’s rib midway between the clinician’s fingers at the distal interphalangeal joint at the center of the patient’s rib and directing superficially (e.g., shallow-deeper-deeper) toward the web-space of the clinician’s hand, versus first needling down to the rib to verify positioning.

Register for Our Course
Myopain Seminars’ curriculum is developed by international leaders in dry needling and manual trigger point therapy. Our courses are a great way to bring a unique and innovative treatment option to your patients. Completing our course programs elevates your practice and expands your clinician’s toolbox to encompass a wide range of therapies that can effectively eliminate patient pain.
References
- Brady S, McEvoy J, Dommerholt J, Doody C. Adverse events following trigger point dry needling: A prospective survey of chartered physiotherapists. J Man Manip Ther. 2013;22:134-40
- McCutcheon L, Yelland M. Iatrogenic pneumothorax: Safety concerns when using acupuncture or dry needling in the thoracic region. PT Rev. 2013;16:126-32
- Witt CM, Pach D, Brinkhaus B, Wruck K, Tag B, Mank S, et al. Safety of acupuncture: Results of a prospective observational study with 229, 230 patients and introduction of a medical information and consent form. Forsch Komplementmed. 2009;16:91-7
- Jung JW, et al. Cardiac tamponade following ultrasonography-guided trigger point injection. 2014: 22:389-391.
- Cushman DM, Scholl LV, Ludlow M, Cunningham S, Teramoto M. Accuracy of rib palpation for dry needling of deep periscapular musculature, measured with ultrasound. J Bodyw Mov Ther. 2021;26:7-11
- Ball AM, Ball EE, Satriano R, Stokes J. Participatory action imaging in increasing clinician confidence of trigger point dry needling or trigger point injection of muscles requiring use of intercostal blocking: A case report. Am J Interv Radiol 2021;5:10
{kind=link}