Dry Needling the Serratus Posterior Superior and Rhomboid Muscles
Once upon a time…actually, not all that long ago, the serratus posterior superior and rhomboid muscles were thought to be difficult muscles to needle because of the congested area between the spine and scapula and the thick overlaying trapezius muscle. Indeed, the muscles present a challenge not only for dry needling and trigger point injections (Fernández de las Peñas, Layton, and Dommerholt 2015) but also for electromyography (Kim et al. 2018). Their proximity to the ribs, especially for the deeper serratus posterior superior, poses a significant risk of pneumothorax (Valera-Calero et al. 2021). Using the intrascapular ribs as an anatomical barrier or backdrop is not recommended as in a recent study, two experienced physical therapists demonstrated only 73.3% accurate palpation of a thoracic rib in the intrascapular region (Cushman et al. 2021).
Taketa and colleagues described performing trigger point injections in the serratus posterior superior muscle using real-time ultrasound guidance (Taketa, Irisawa, and Fujitani 2018). Dry needling these muscles is, however, surprisingly easy and safe even without ultrasound guidance by using the so-called “downhill” technique developed by Dr. Jan Dommerholt.
Muscle Anatomy and Referred Pain Patterns
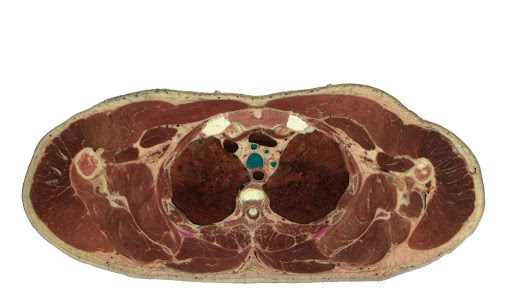
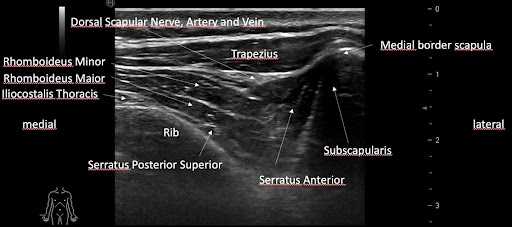
It would seem impossible to differentiate between the rhomboid muscles and the serratus posterior superior with palpation. Both muscles are very thin and are covered by the trapezius. Looking at the muscles with sonography, Belgian sports medicine physician Dr. Kris Demanet confirms how thin the serratus posterior superior really is. To think that this muscle can be identified by palpation seems to be fictitious.
Yet, Simon, Travell, and Simons described two completely different referred pain patterns (Simons, Travell, and Simons 1999) suggesting that accurate differentiation would be possible. They described the pain pattern of the rhomboids referring intrascapularly and into the posterior shoulder, while the pain pattern for the serratus posterior superior would extend all the way through the arm into the fingers.
Rhomboids – Anatomy and Referred Pain Pattern


Serratus Posterior Superior – Anatomy and Referred Pain Pattern


Case 1 by Dr. Rob Stanborough
History and Symptoms: A Male With Numbness in Both Hands
A thirty-four-year-old male special forces officer in the United States Army presented with numbness in both hands. Every night, about two hours after falling asleep, he would awake with numbness in both hands, the numbness in his right hand being slightly more than in his left hand. After waking, he would shake his hands without any change, reposition himself, and try to go back to sleep. He had no history of trauma to his neck, shoulders, or arms, and answered his medical questionnaire as follows:
Question: “Work-related or recreational activities you participate in regularly?”
Answer: “A lot”.
As a computer analyst, he would sit for long periods of time, but he did not experience hand numbness when doing so. Because his sleep was interrupted so regularly, he stated it was affecting his ability to concentrate and work.
He had been sent for a cervical MRI, which was unremarkable.
Examination: Mobility and Myofascial Trigger Points
The patient presented with good posture with slightly rounded shoulders. Examining his neck first, he was able to demonstrate full flexion/extension, side-bending right, side-bending left, and rotation right and left without any limitation or symptom reproduction. He presented with a limitation in shoulder flexion, R>L, and decreased bilateral internal and external rotation, due to muscle tightness but without symptom reproduction. The accessory mobility of his sub-cranial, cervical, and thoracic spine revealed hypomobility, believed to be from muscle guarding more than joint stiffness. His shoulder accessory mobility was normal. His elbows were unremarkable with a screen, and he presented with no limitations in wrist flexion/extension, radial or ulnar deviation. Neural tension of the upper extremity was also negative for the median, radial, and ulnar nerves, so no special tests were performed at the wrist for median nerve entrapment.
Because all suspected sources of mechanical failure had been tested and his symptoms were still not reproduced, myofascial trigger points were examined. Trigger points in the infraspinatus were found to be exquisitely painful but did not reproduce pain in the hands.
Treatment One: Initial Dry Needling Approach
Treatment was initiated by treating each infraspinatus with dry needling. The rhomboids were treated next based on his slightly rounded shoulders and scapular protraction, using the downhill approach. With this approach, the needle is directed perpendicular to the thoracic ribs at a shallow angle. Recommended needle length is 50 mm or more. During the dry needling procedure, the patient experienced local twitch responses and responded with a “jump sign.” The needle did not touch the ribs. Following dry needling, moderate pressure and soft tissue manipulation were applied to each of these muscles. The patient was given scapular squeezes and doorway stretches as a HEP.




Downhill Approach for Needling the Rhomboids and Serratus Posterior Superior
Treatment Two: Dry Needling With a 60mm Needle
The patient returned stating the numbness was unchanged. Treatment was applied similarly to the first treatment, but with one important difference. In the second treatment, when the rhomboids were treated because the interscapular muscles were so thick and developed, Dr. Stanborough used a 60 mm needle and in doing so, he was able to angle the needle deeper without danger of causing a pneumothorax. In fact, on a few occasions, the ribs were hit with the needle.
Upon the deeper, tangential (downhill) application, the patient indicated feeling symptoms in his hands, right on right and left on left. He experienced multiple twitch responses on both sides. When the needling was completed and all local twitch responses were eliminated, soft tissue manipulation was applied. The patient was asked to roll over and lie on his back as this was the position whereby, he experienced most numbness in the hands. After waiting 10 minutes, the patient still reported no numbness.
Treatment Three: Follow-Up Appointment
Following treatment two, the patient left town for five weeks due to work. Upon return he called for a follow-up appointment. He reported that all numbness had been resolved after the second treatment. He returned for a follow-up visit because he was beginning to experience “just a little bit” in the left hand. The infraspinatus, rhomboids, and serratus posterior superior muscles were treated one more time. Soft tissue manipulation was applied and the use of a foam roller for self-treatment was reviewed.
The patient had to leave town again for several weeks but did report the foam roller helped and he was able to self-treat his posterior shoulder muscles.
Case 2 by Dr. Jan Dommerholt
History and Symptoms: A Student With Pain in His Left Hand
An 18-year high school student presented with pain in his left hand when playing the contrabass with the left hand near the bottom of the neck of the instrument over the so-called upper bout.
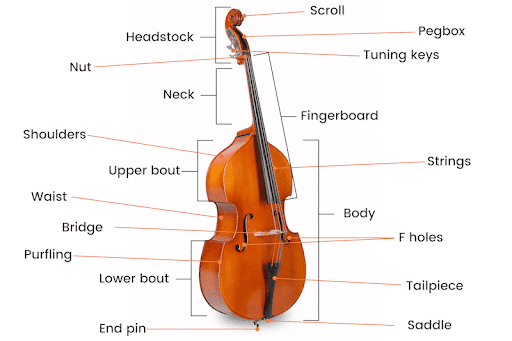
When he played higher on the neck, he experienced no symptoms at all. The patient was rather concerned about this immediate onset of left-sided hand pain as he was preparing multiple recordings as part of the application process to attend a music conservatorium or performing art school. He was worried about what this pain would mean for his desire to become a professional musician.
Since he did not have pain in his hand when he was not playing the double bass, he was classified as a grade 1 on the Functional Grading of Severity of Injury (Dommerholt 2009; Fry 1986). The Functional Grading of Severity of Injury scale can be used to document a musician’s status at intake and measure the progress of therapeutic interventions. Although the scale has not been validated, it is frequently used by performing arts medicine practitioners (Hoppmann and Patrone 1989). While a score of a grade 1 is not life-threatening, even such a low score can be career-threatening for musicians and may seriously impact their ability to play their instruments.
Functional Grading of Severity of Injury
Examination: Palpation and Observation
Although the patient did not describe experiencing intrascapular pain, part of the initial examination included palpation of the rhomboid/serratus posterior superior muscles. With prolonged manual pressure over a trigger point in these muscles, the patient reported the onset of pain in his left forearm and hand. The onset of referred pain would suggest the involvement of the serratus posterior superior muscle, however, from a more mechanical point of view, the action of reaching to the bottom of the neck of the instrument would be more likely to involve the rhomboid muscles. The initial physical therapy evaluation included observations and analysis of playing the double bass.
Treatment: Dry Needling Using the Downhill Approach
The patient was treated with dry needling of the rhomboids/serratus posterior superior muscles using the downhill approach. Local twitch responses were elicited and the onset of a pain sensation in the left hand. The treatment was concluded with soft tissue mobilization of the involved muscles. Following the treatment, the patient did not experience any pain with playing the bass in any position on the neck. Two weeks later, he was still symptom-free despite an increased playing schedule due to the recital preparations.
Conclusions From the Two Cases
The significance of these cases is twofold. In the clinic, the serratus posterior superior muscle and its referred pain pattern into the hands can be easily overlooked. Although the term “referred pain” would be appropriate for the musician (case 2), the patient in the first case did not experience any referred pain. A Delphi study published in 2018 by Fernández-de-la-Peñas and Dommerholt revealed that the term “referred sensation” was indeed preferred by 60 healthcare providers from 12 countries (Fernández-De-Las-Peñas and Dommerholt 2018).
Even though it is tempting to conclude that when a twitch response occurs right before touching the rib with the needle, it must follow that the serratus posterior superior was needled, one can never be 100% sure given the anatomical characteristics of the muscle and the rhomboids. In the first case, the symptoms resolved with the deeper needling approach suggesting that indeed the serratus posterior superior was needled. In the second case, the pain pattern suggested the involvement of the serratus posterior superior, but the mechanical action suggested that the rhomboids were the culprit.
Secondly, the downhill approach recommended by Myopain Seminars is indeed a safe and beneficial technique even when treating a deep muscle like the serratus posterior superior or the slightly more superficial rhomboids.
References
- Cushman, Daniel M., Linda Vernon Scholl, Monica Ludlow, Shellie Cunningham, and Masaru Teramoto. 2021. “Accuracy of rib palpation for dry needling of deep periscapular musculature, measured with ultrasound.” Journal of Bodywork and Movement Therapies 26:
- Dommerholt, J. 2009. “Performing arts medicine – instrumentalist musicians part I – general considerations.” J Bodyw Mov Ther 13 (4):311-9. doi: 10.1016/j.jbmt.2009.02.003.
- Dor, A., J. J. Vatine, and L. Kalichman. 2019. “Proximal myofascial pain in patients with distal complex regional pain syndrome of the upper limb.” J Bodyw Mov Ther 23 (3):547-554. doi: 10.1016/j.jbmt.2019.02.015.
- Fernandez-de-Las-Penas C, Layton M, Dommerholt J. 2015. Dry needling for the management of thoracic spine pain. J Manual Manipulative Ther. 23(3):147-53. doi: 10.1179/2042618615Y.0000000001
- Fernández-De-Las-Peñas, C., and J. Dommerholt. 2018. “International Consensus on Diagnostic Criteria and Clinical Considerations of Myofascial Trigger Points: A Delphi Study.” Pain Med 19 (1):142-150. doi: 10.1093/pm/pnx207.
- Fry, J.H.H. 1986. “Overuse syndrome of the upper limb in musicians.” Med J Australia 144:182-185.
- Hoppmann, R. A., and N. A. Patrone. 1989. “A review of musculoskeletal problems in instrumental musicians.” Semin Arthritis Rheum 19 (2):117-26. doi: 0049-0172(89)90056-5 [pii].
- Kim, K. H., G. Y. Kim, S. G. Lim, B. K. Park, and D. H. Kim. 2018. “A More Precise Electromyographic Needle Approach for Examination of the Rhomboid Major.” PM R 10 (12):1380-1384. doi: 10.1016/j.pmrj.2018.05.009.
- Simons, D.G., J.G. Travell, and L.S. Simons. 1999. Travell and Simons’ myofascial pain and dysfunction; the trigger point manual. 2 ed. Vol. 1. Baltimore: Williams & Wilkins.
- Taketa, Y., Y. Irisawa, and T. Fujitani. 2018. “Ultrasound guided serrates posterior superior muscle block relieves interscapular myofascial pain.” J Clin Anesth 44:10-11. doi:10.1016/j.jclinane.2017.10.009.
- Valera-Calero, J. A., E. Cendra-Martel, T. Fernandez-Rodriguez, C. Fernandez-de-Las-Penas, G. M. Gallego-Sendarrubias, and J. Guodemar-Perez. 2021. “Prediction model of rhomboid major and pleura depth based on anthropometric features to decrease the risk