




Beyond the Haystack: Optimizing Trigger Point Identification
 Trigger point dry needling (TrP-DN) is a powerful tool, but its effectiveness hinges greatly on precise TrP identification. However, simply diving into palpation based solely on a patient’s pain complaints is akin to searching for a needle in a haystack – inefficient and time-consuming. Texts on myofascial pain suggest more than 20 muscles that could potentially refer symptoms to the shoulder (Donnelly et al, 2019). Palpating every single one of those muscles in a treatment session is just not practical, especially when some of those muscles can be as large as the latissimus dorsi. A little detective work before your palpation goes a long way toward efficient and effective treatment.
Trigger point dry needling (TrP-DN) is a powerful tool, but its effectiveness hinges greatly on precise TrP identification. However, simply diving into palpation based solely on a patient’s pain complaints is akin to searching for a needle in a haystack – inefficient and time-consuming. Texts on myofascial pain suggest more than 20 muscles that could potentially refer symptoms to the shoulder (Donnelly et al, 2019). Palpating every single one of those muscles in a treatment session is just not practical, especially when some of those muscles can be as large as the latissimus dorsi. A little detective work before your palpation goes a long way toward efficient and effective treatment.
A comprehensive examination, encompassing both subjective and objectiv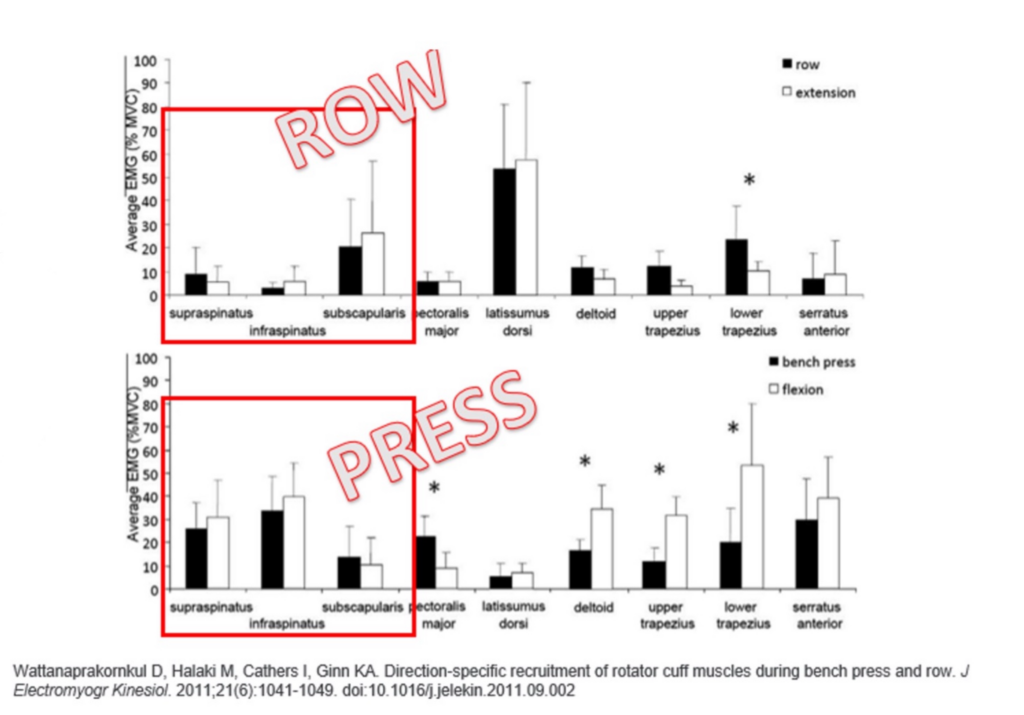 e assessments, paves the way for efficient palpation. This includes talking with your patients and watching them move. The history is a goldmine of information! Aim to truly understand what makes the symptoms worse and what eases them. Certain stimuli (positions/movements) will stress some muscles more than others. If a muscle has a relevant TrP, a stronger stimulus to that muscle may lead to a stronger reproduction of symptoms. For example, lateral shoulder pain, strongly aggravated during pressing movements, implicates the infraspinatus more than the subscapularis. The rotator cuff muscles dynamically stabilize the glenohumeral joint, but not all shoulder motions elicit the same level of EMG activity throughout the cuff. Research of nine different shoulder muscles shows that the infraspinatus has the highest EMG activity of any of the measured muscles during horizontal pressing (including the subscapularis and supraspinatus), which contrasts with pulling movements where the subscapularis becomes much more active than the infraspinatus (Wattanaprakornkul, 2011).
e assessments, paves the way for efficient palpation. This includes talking with your patients and watching them move. The history is a goldmine of information! Aim to truly understand what makes the symptoms worse and what eases them. Certain stimuli (positions/movements) will stress some muscles more than others. If a muscle has a relevant TrP, a stronger stimulus to that muscle may lead to a stronger reproduction of symptoms. For example, lateral shoulder pain, strongly aggravated during pressing movements, implicates the infraspinatus more than the subscapularis. The rotator cuff muscles dynamically stabilize the glenohumeral joint, but not all shoulder motions elicit the same level of EMG activity throughout the cuff. Research of nine different shoulder muscles shows that the infraspinatus has the highest EMG activity of any of the measured muscles during horizontal pressing (including the subscapularis and supraspinatus), which contrasts with pulling movements where the subscapularis becomes much more active than the infraspinatus (Wattanaprakornkul, 2011).
So, if your patient tells you that pushing open a door is painful, where pulling it open is not, you may want to prioritize palpating the infraspinatus over the subscapularis. This can be applied to non-rotator cuff muscles that refer to the shoulder, such as the latissimus dorsi, which is much more active during pulling versus pressing motions.
Corroborating the subjective history with your objective examination is key. A thorough movement exam can be a game-changer. For a patient report of anterior shoulder pain during active flexion, carefully watch them do the activity. Is the pain due to poor motor control? Restricted range of motion? A TrP in the latissimus dorsi could cause anterior shoulder pain. If the patient flexes their arm and hits a barrier, this may stimulate the latissimus dorsi TrP and potentially cause pain. Conversely, if there’s no flexibility limitation and the pain stems from an infraspinatus trigger point, passive flexion will not likely be painful, whereas active flexion likely will be.
Multiple TrPs can exist within a region, and incidental findings during palpation might not be the primary driver of the patient’s symptoms. By correlating your palpation findings with the subjective history and movement exam, you can more efficiently and effectively differentiate between “noise” and the true trigger points responsible for the patient’s dysfunction.
A Few References
- Donnelly, J., Fernández-de-Las-Peñas, C., Finnegan, M., & Freeman, J. F. (2019). Travell, Simons & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual (Vol. 3). Wolters Kluwer.
- Wattanaprakornkul D, Halaki M, Cathers I, Ginn KA. Direction-specific recruitment of rotator cuff muscles during bench press and row. J Electromyogr Kinesiol. 2011;21(6):1041-1049.
Myopain Seminars Course Series

The Dry Needling 1 course is an excellent starting point for learning the fundamentals of dry needling therapy. With a focus on the safe and effective application of dry needling techniques, you will gain a solid understanding of myofascial trigger points, needling techniques, precautions, and how to apply these techniques in clinical practice.

The MTT-1 course includes an introduction to the history of trigger points and myofascial pain. Many muscles commonly encountered in clinical practice will be addressed, including the trapezius, levator scapula, pectoralis major and minor, posterior neck and sub-occipital muscles, quadratus lumborum, iliacus and psoas, tensor fascia lata, sartorius, quadriceps, hamstrings, gastrocnemius, soleus, plantaris, and popliteus muscles, among many others.

The Fu Subcutaneous Needling – American Version Course (FSN) offers a comprehensive introduction to fascial needling by areas of the body and incorporates prior learning of myofascial pain, trigger points, and referral patterns, and unique needling techniques. FSN is a great addition to the practitioner’s toolbox to offer a safe and effective treatment option with minimal discomfort for the patient.
{kind=link}