



Body Image and Distorted Perception of One’s Own Body – What Does This Mean?
Body Image (BI): A Multifaceted Perception
 Body Image (BI) refers to how individuals subjectively perceive their own bodies, which often diverges from their actual physical form. This perception is a complex amalgam of one’s thoughts, feelings, evaluations, and behaviors related to their body. Clinically, the significance of BI stems from its linkage to various severe disorders such as body dysmorphic disorder, anorexia nervosa, and bulimia nervosa. BI’s Disturbances can profoundly affect physical and psychological health, influencing factors like self-esteem, mood, social interaction, and job performance. These distortions, characterized by altered perceptions and attitudes towards the body, can result in negative experiences and outcomes, thereby underscoring the necessity for a comprehensive understanding of normal and abnormal body image perceptions for effective intervention (Hosseini & Padhy, 2022).
Body Image (BI) refers to how individuals subjectively perceive their own bodies, which often diverges from their actual physical form. This perception is a complex amalgam of one’s thoughts, feelings, evaluations, and behaviors related to their body. Clinically, the significance of BI stems from its linkage to various severe disorders such as body dysmorphic disorder, anorexia nervosa, and bulimia nervosa. BI’s Disturbances can profoundly affect physical and psychological health, influencing factors like self-esteem, mood, social interaction, and job performance. These distortions, characterized by altered perceptions and attitudes towards the body, can result in negative experiences and outcomes, thereby underscoring the necessity for a comprehensive understanding of normal and abnormal body image perceptions for effective intervention (Hosseini & Padhy, 2022).
Somatorepresentation and its Distortions
Somatorepresentation concerns how individuals perceive and represent their bodily sensory and motor functions. In musculoskeletal disorders, distortions in somato-representation are evident, affecting epicritic sensitivity (such as tactile acuity) and discriminative abilities. Chronic musculoskeletal disorders frequently present these abnormalities, including reduced two-point discrimination, sensorimotor deficits, and modified emotional processing. In this musculoskeletal context, somatosensory abnormalities like diminished tactile acuity, impaired laterality recognition, and affected facial emotion recognition are noticeable. These represent a blend of cognitive, perceptive, and affective issues, indicating the critical role of multisensory integration in such sensory distortions (Stanton et al., 2013).
 From a musculoskeletal perspective, we need to consider somatosensory irregularities, especially in areas like epicritic and discriminative sensitivity, which include tactile acuity often assessed through two-point discrimination tests (von Piekartz & Paris-Alemany, 2021). Left-right recognition (LAT) and facial emotion recognition (FER) are mental imagery tasks. Disruptions in these areas can indicate face-related emotional and physical impairments, encompassing cognitive, perceptual, and affective elements (Hosseini & Padhy, 2022; Parsons, 1987).
From a musculoskeletal perspective, we need to consider somatosensory irregularities, especially in areas like epicritic and discriminative sensitivity, which include tactile acuity often assessed through two-point discrimination tests (von Piekartz & Paris-Alemany, 2021). Left-right recognition (LAT) and facial emotion recognition (FER) are mental imagery tasks. Disruptions in these areas can indicate face-related emotional and physical impairments, encompassing cognitive, perceptual, and affective elements (Hosseini & Padhy, 2022; Parsons, 1987).
Research shows that individuals with chronic musculoskeletal conditions frequently exhibit somatosensory issues, such as a lack of two-point discrimination (Catley, Tabor, Wand, & Moseley, 2013; Luedtke et al., 2018; Luomajoki & Moseley, 2011; Maarbjerg et al., 2017; Stanton et al., 2013), along with sensorimotor deficits (in LAT, movement control) (Breckenridge et al., 2015; Elsig et al., 2014; Linder, Michaelson, & Roijezon, 2016; Reinersmann et al., 2010), and changed emotional processing (FER, alexithymia) (Aaron, Fisher, de la Vega, Lumley, & Palermo, 2019; Di Tella & Castelli, 2016; Piekartz, Wallwork, Mohr, Butler, & Moseley, 2015; von Piekartz & Mohr, 2014).
Patients with chronic orofacial pain often report feeling as if the painful area of their face is “swollen,” even when there are no clinical signs of swelling, a clear indication of perceptual distortion. Even administering local anesthetics in healthy individuals can lead to similar perceptions. This suggests that multisensory integration plays a crucial role in this type of sensory distortion and could be key to understanding the factors influencing this common condition (Dagsdóttir et al., 2018).
Somatorepresentation in Orofacial Pain
With a prevalence of 10%-15% and an annual incidence of about 5% in the adult population, orofacial pain syndromes like temporomandibular disorders belong to the most common musculoskeletal disorders (LeResche, 1997; Lipton et al., 1993). As already described with orofacial pain, distortions of somato-representation can be observed with similar body image distortions (von Piekartz & Paris-Alemany, 2021). These aspects can be divided into the following parts. We also included the option to test specific motor and somatosensory disturbances:
- Tactile acuity is tested mainly with so-called two-point discrimination. Studies show changes in this somatosensory component in TMD and migraine (La Touche et al., 2020; Luedtke et al., 2018).

- Auditory acuity involves localizing sounds and pitches and muting background noises (Stamper & Johnson, 2015). Using a speaker with variable frequencies (250–8000 Hz) and sound intensities (5–40 dB), measuring different regions of the so-called peripersonal space is possible (Figure 1)
-
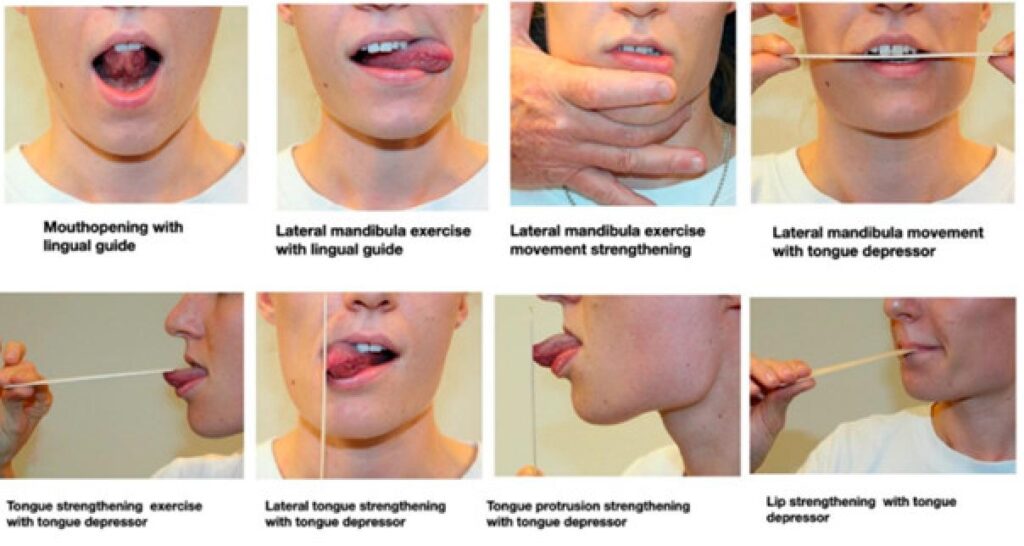
Figure 2 – Facial motor exercises (from von Piekartz and Paris-Alemany, 2021 Laterality recognition: special programs, like the CRAFTA® face-training program, test the ability to recognize left or right body parts or body movements (von Piekartz et al., 2017). Accuracy and reaction time are proper objective parameters to evaluate a progression in the rehabilitation of orofacial pain syndromes.
- Motor control disturbances are already recognized in lumbar and cervical spine disorders, but motor control assessment and evaluation also should be an integral part of any orofacial rehabilitation program. Standardized movement control exercises can also be assessed and trained, whereas mirror therapy plays an important role in rehabilitation (Figures 2 & 3).

Psychological and emotional components
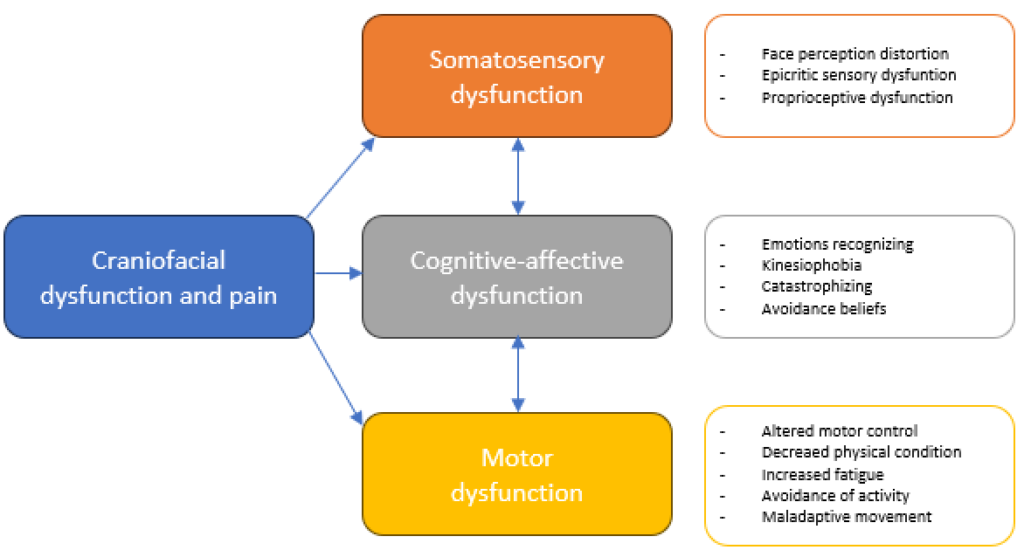
Adopting a biopsychosocial approach within the CRAFTA® framework, it is crucial to acknowledge and address cognitive and emotional disturbances to understand and treat a patient’s issue comprehensively. There are notable links between the aforementioned disorders and various psychological and emotional factors. These include catastrophizing, fear-avoidance behaviors, kinesiophobia, difficulties in recognizing facial emotions, alexithymia, as well as depression and anxiety. These psychological states can lead to sleep disturbances and overall physical deconditioning (Haas et al., 2013; Kindler et al., 2018; Lei et al., 2015; Pedrosa Gil et al., 2008; Slade et al., 2016). It is important to remember that addressing these psychological dimensions often requires specialized professionals, such as psychologists, psychiatrists, or psychotherapists because there are significant connections between somatosensory and sensorimotor issues and these emotional, cognitive-affective aspects.
The following chart illustrates the dysfunctional aspects of craniofacial pain and their corresponding dysfunctions or distortions, which align with the knowledge presented.
Topics included in the training of a CRAFTA®-Certified Physical Therapist
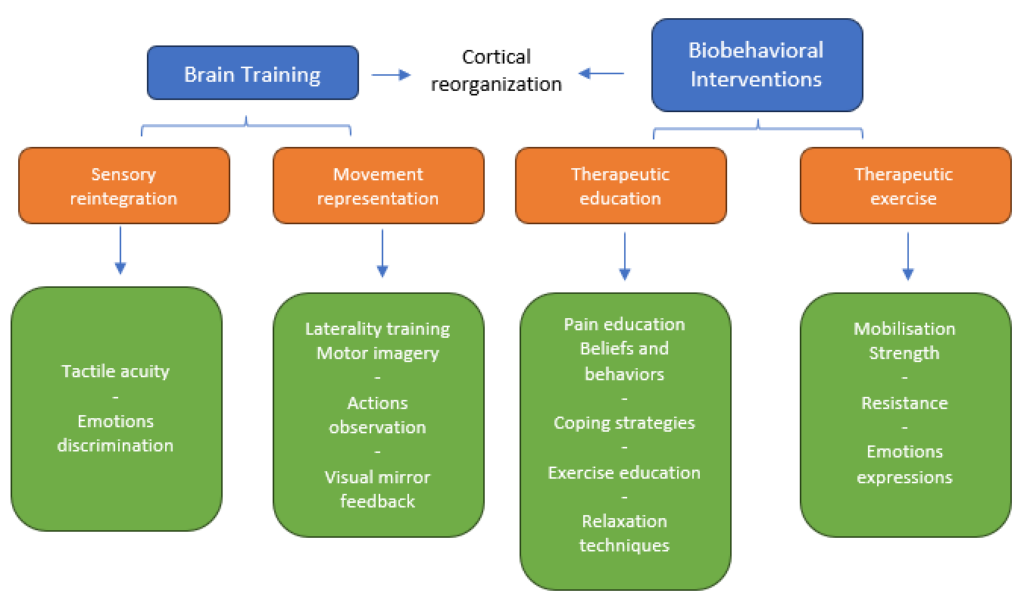
The CRAFTA courses cover two primary strategies, including brain training and biobehavioral interventions, with four key elements in the assessment and treatment protocol.
- somatosensory reintegration (tactile and discriminative),
- movement representation techniques,
- therapeutic exercise (motor training),
- therapeutic patient education (to reinforce the other interventions from a behavioral point of view).
In the CRAFTA® training program, participants begin by learning to evaluate and assess orofacial conditions from a comprehensive point of view, incorporating both structural and functional assessments, such as
- The application of manual techniques and motor control elements aids in reducing somatosensory distortions.
- Advanced courses delve into body image considerations, explore motor control exercises, and discuss pain management strategies and the implementation of graded activity methods.
- Topics like facial emotion recognition and laterality are covered in the advanced courses.
- Additionally, a specific online course aligns with a unique app developed for this purpose.
Bernhard Taxer, PhD, MSc PT, MT (OMPT) and Harry von Piekartz, PhD, MSc, PT, MT (OMPT)
References:
Aaron, R. V., Fisher, E. A., de la Vega, R., Lumley, M. A., & Palermo, T. M. (2019). Alexithymia in individuals with chronic pain and its relation to pain intensity, physical interference, depression, and anxiety: a systematic review and meta-analysis. Pain, 160(5), 994-1006. https://doi.org/10.1097/j.pain.0000000000001487
Breckenridge, J. D., McAuley, J. H., Butler, D. S., Stewart, H., Moseley, G. L., & Ginn, K. A. (2015). Shoulder left/right judgment task: development and establishment of a normative dataset. Physiotherapy, 101, e169-e170. https://doi.org/10.1016/j.physio.2015.03.323
Catley, M. J., Tabor, A., Wand, B. M., & Moseley, G. L. (2013). Assessing tactile acuity in rheumatology and musculoskeletal medicine–how reliable are two-point discrimination tests at the neck, hand, back and foot? Rheumatology (Oxford), 52(8), 1454-1461. https://doi.org/10.1093/rheumatology/ket140
Dagsdóttir, L. K., Bellan, V., Skyt, I., Vase, L., Baad-Hansen, L., Castrillon, E., & Svensson, P. (2018). Multisensory modulation of experimentally evoked perceptual distortion of the face. J Oral Rehabil, 45(1), 1-8. https://doi.org/10.1111/joor.12581
Di Tella, M., & Castelli, L. (2016). Alexithymia in Chronic Pain Disorders. Curr Rheumatol Rep, 18(7), 41. https://doi.org/10.1007/s11926-016-0592-x
Elsig, S., Luomajoki, H., Sattelmayer, M., Taeymans, J., Tal-Akabi, A., & Hilfiker, R. (2014). Sensorimotor tests, such as movement control and laterality judgment accuracy, in persons with recurrent neck pain and controls. A case-control study. Man Ther, 19(6), 555-561. https://doi.org/10.1016/j.math.2014.05.014
Haas, J., Eichhammer, P., Traue, H. C., Hoffmann, H., Behr, M., Crönlein, T., Pieh, C., & Busch, V. (2013). Alexithymic and somatisation scores in patients with temporomandibular pain disorder correlate with deficits in facial emotion recognition. Journal of Oral Rehabilitation, 40(2), 81–90. https://doi.org/10.1111/joor.12013
Hosseini, S. A., & Padhy, R. K. (2022). Body Image Distortion. In StatPearls. Treasure Island (FL): StatPearls Publishing.
Kindler, S., Schwahn, C., Terock, J., Mksoud, M., Bernhardt, O., Biffar, R., Völzke, H., Metelmann, H. R., & Grabe, H. J. (2018). Alexithymia and temporomandibular joint and facial pain in the general population. Journal of Oral Rehabilitation. https://doi.org/10.1111/joor.12748
La Touche, R., Cuenca-Martínez, F., Suso-Martí, L., García-Vicente, A., Navarro-Morales, B., & Paris-Alemany, A. (2020). Tactile trigeminal region acuity in temporomandibular disorders: A reliability and cross-sectional study. Journal of Oral Rehabilitation, 47(1), 9–18. https://doi.org/10.1111/joor.12870
Lei, J., Liu, M.-Q., Yap, A. U. J., & Fu, K.-Y. (2015, March 30). Sleep Disturbance and Psychologic Distress: Prevalence and Risk Indicators for Temporomandibular Disorders in a Chinese Population. https://doi.org/10.11607/ofph.1301
LeResche, L. (1997). Epidemiology of temporomandibular disorders: Implications for the investigation of etiologic factors. Critical Reviews in Oral Biology and Medicine: An Official Publication of the American Association of Oral Biologists, 8(3), 291–305. https://doi.org/10.1177/10454411970080030401
Lipton, J., Ship, J., & Larach-Robinson, D. (1993). Estimated Prevalence and Distribution of Reported Orofacial Pain in the United States. The Journal of the American Dental Association, 124(10), 115–121. https://doi.org/10.14219/jada.archive.1993.0200
Linder, M., Michaelson, P., & Roijezon, U. (2016). Laterality judgments in people with low back pain–A cross-sectional observational and test-retest reliability study. Man Ther, 21, 128-133. https://doi.org/10.1016/j.math.2015.07.001
Luedtke, K., Adamczyk, W., Mehrtens, K., Moeller, I., Rosenbaum, L., Schaefer, A., . . . Wollesen, B. (2018). Upper cervical two-point discrimination thresholds in migraine patients and headache-free controls. Journal of Headache & Pain, 19(1), 47. https://dx.doi.org/10.1186/s10194-018-0873-z
Luomajoki, H., & Moseley, G. L. (2011). Tactile acuity and lumbopelvic motor control in patients with back pain and healthy controls. Br J Sports Med, 45(5), 437-440. https://doi.org/10.1136/bjsm.2009.060731
Maarbjerg, S., Wolfram, F., Heinskou, T. B., Rochat, P., Gozalov, A., Brennum, J., . . . Bendtsen, L. (2017). Persistent idiopathic facial pain – a prospective systematic study of clinical characteristics and neuroanatomical findings at 3.0 Tesla MRI. Cephalalgia, 37(13), 1231-1240. https://doi.org/10.1177/0333102416675618
Parsons, L. M. (1987). Imagined spatial transformations of one’s hands and feet. Cogn Psychol, 19(2), 178-241. https://doi.org/10.1016/0010-0285(87)90011-9
Pedrosa Gil, F., Ridout, N., Kessler, H., Neuffer, M., Schoechlin, C., Traue, H. C., & Nickel, M. (2008). Facial emotion recognition and alexithymia in adults with somatoform disorders. Depression and Anxiety, 25(11), E133–E141. https://doi.org/10.1002/da.20440
Piekartz, H., Wallwork, S. B., Mohr, G., Butler, D. S., & Moseley, G. L. (2015). People with chronic facial pain perform worse than controls at a facial emotion recognition task, but it is not all about the emotion. Journal of Oral Rehabilitation, 42(4), 243-250. https://doi.org/10.1111/joor.12249
Reinersmann, A., Haarmeyer, G. S., Blankenburg, M., Frettloh, J., Krumova, E. K., Ocklenburg, S., & Maier, C. (2010). Left is where the L is right. Significantly delayed reaction time in limb laterality recognition in both CRPS and phantom limb pain patients. Neurosci Lett, 486(3), 240-245. https://doi.org/10.1016/j.neulet.2010.09.062
Slade, G. D., Ohrbach, R., Greenspan, J. D., Fillingim, R. B., Bair, E., Sanders, A. E., Dubner, R., Diatchenko, L., Meloto, C. B., Smith, S., & Maixner, W. (2016). Painful Temporomandibular Disorder. Journal of Dental Research, 95(10), 1084–1092. https://doi.org/10.1177/0022034516653743
Stamper, G. C., & Johnson, T. A. (2015). Auditory Function in Normal-Hearing, Noise-Exposed Human Ears. Ear and Hearing, 36(2), 172. https://doi.org/10.1097/AUD.0000000000000107
Stanton, T. R., Lin, C. W., Bray, H., Smeets, R. J., Taylor, D., Law, R. Y., & Moseley, G. L. (2013). Tactile acuity is disrupted in osteoarthritis but is unrelated to disruptions in motor imagery performance. *Rheumatology (Oxford), 52*(8), 1509-1519. doi:10.1093/rheumatology/ket139
von Piekartz, H., & Mohr, G. (2014). Reduction of head and face pain by challenging lateralization and basic emotions: a proposal for future assessment and rehabilitation strategies. *Journal of Manual & Manipulative Therapy (Maney Publishing), 22*(1), 24-35. doi:10.1179/2042618613Y.0000000063
von Piekartz, H., Lüers, J., Daumeyer, H., & Mohr, G. (2017). [Is kinesiophobia associated with changes in left/right judgment and emotion recognition during a persisting pain condition? : A cross-sectional study]. *Schmerz (Berlin, Germany), 31*(5), 483–488. https://doi.org/10.1007/s00482-017-0220-3
von Piekartz, H., & Paris-Alemany, A. (2021). Assessment and Brain Training of Patients Experiencing Head and Facial Pain with a Distortion of Orofacial Somatorepresentation: A Narrative Review. *Applied Sciences, 11*(15),Retrieved from https://www.mdpi.com/2076-3417/11/15/6857
{kind=link}